
Is Cervical Endoscopic Discectomy Right for Me?

Neck pain that radiates into the shoulder, arm, or hand can significantly interfere with daily life. For some patients, symptoms improve with physical therapy, medications, or injections. But when pain, numbness, or weakness continue despite conservative treatment, surgery may become an option. One minimally invasive procedure gaining attention is cervical endoscopic discectomy — an advanced technique designed to relieve nerve compression while minimizing disruption to surrounding tissues.
But how do you know if it is the right procedure for you?
If your symptoms — such as arm pain, numbness, weakness, or neck pain — are caused by a cervical disc herniation confirmed on MRI, and conservative treatments are no longer helping, cervical endoscopic discectomy may be worth discussing with a spine specialist.
The key is ensuring that:
- Your symptoms match the imaging findings
- The anatomy is appropriate for endoscopic treatment
- Conservative care has been adequately explored
- The surgical plan aligns with your goals and condition
Not every patient needs fusion, and not every patient is a candidate for endoscopic surgery. The most important step is choosing the right procedure for the right patient through careful evaluation, imaging review, and individualized treatment planning. Call Empire Spine & Pain Management, we help patients across New York & New Jersey with clinic locations at Plainview, NY • Clifton, NJ • Plainfield, NJ • Montville, NJ • Ronkonkoma, NY • New York, NY • New Hyde Park, NY
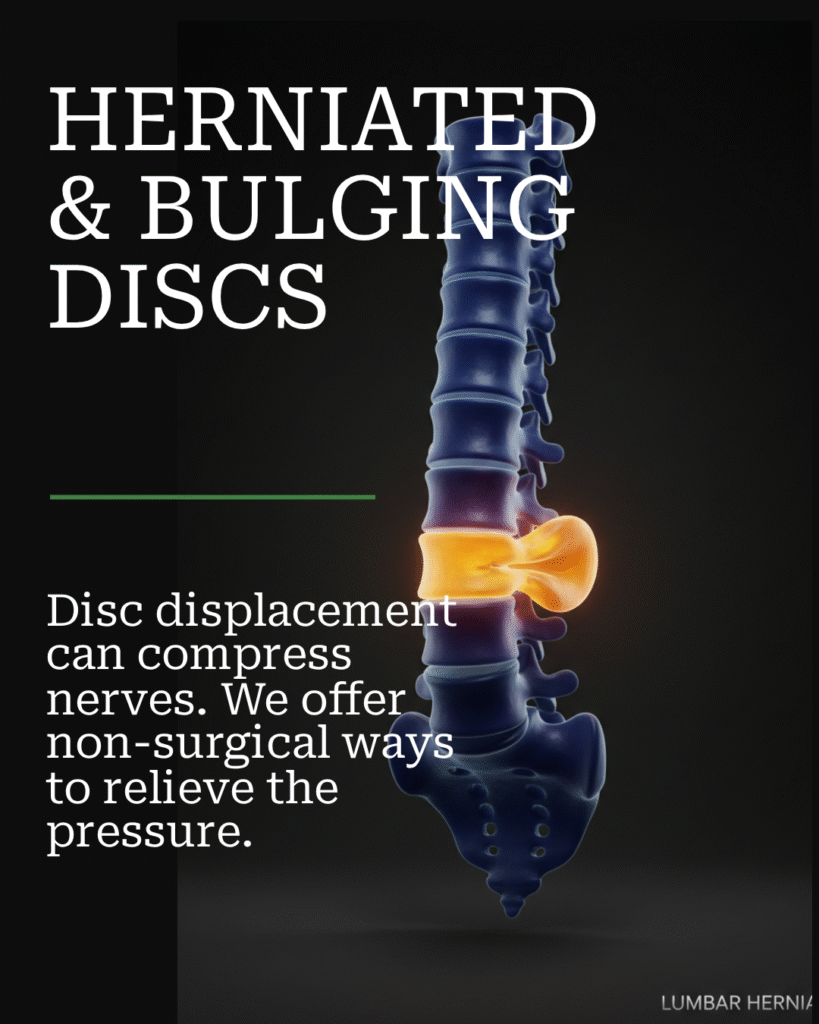
Understanding Cervical Disc Herniation
The cervical spine consists of the seven vertebrae in the neck. Between these bones are discs that act as cushions and help maintain flexibility and motion. When a cervical disc herniates or protrudes, it can compress nearby nerves exiting the spine. This nerve compression may lead to symptoms such as:
- Neck pain
- Shoulder pain
- Arm pain
- Numbness or tingling
- Hand weakness
- Burning or shooting pain down the arm
In many cases, symptoms improve with conservative care. However, persistent nerve compression can continue causing pain and functional limitations when non-surgical treatments no longer provide relief.
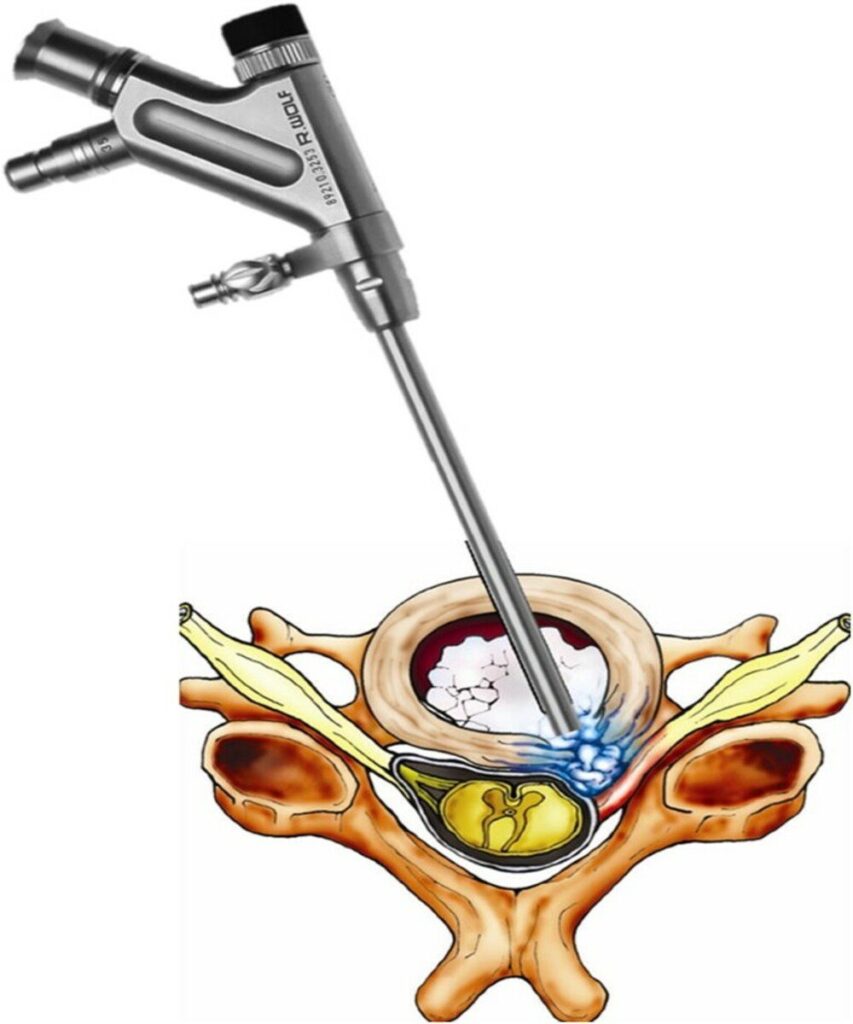
What Is Cervical Endoscopic Discectomy?
Cervical endoscopic discectomy is a minimally invasive spine procedure used to relieve pressure on compressed cervical nerves caused by disc herniations or foraminal stenosis. Using specialized endoscopic technology and small instruments, the surgeon accesses the affected area through a smaller incision compared to traditional open surgery. The goal is targeted nerve decompression while preserving as much normal anatomy as possible. Unlike some traditional cervical procedures, selected patients may avoid fusion, helping preserve motion in the neck.
Who Is a Good Candidate for Cervical Endoscopic Discectomy?
The best candidates are patients with symptoms that clearly correlate with MRI findings showing focal cervical nerve compression. Ideal candidates often experience:
- Neck pain radiating into the arm
- Arm numbness or tingling
- Weakness in the arm or hand
- Persistent symptoms despite conservative treatment
Patients who commonly benefit from this approach include those with:
- One- or two-level soft disc herniations
- Foraminal stenosis
- Focal nerve root compression
- Persistent pain despite therapy, injections, or medications
- A desire to preserve spinal motion when appropriate
One of the most important aspects of candidacy is ensuring that the patient’s symptoms, physical examination, and imaging findings all match. MRI findings alone do not determine whether surgery is appropriate.
Who May Not Be a Candidate?
While cervical endoscopic discectomy can be highly effective for properly selected patients, not everyone is an ideal candidate. Patients who may require alternative procedures include those with:
- Severe spinal instability
- Advanced spinal cord compression (myelopathy)
- Extensive calcified disc disease
- Severe spinal deformity
- Advanced multilevel degeneration
- Symptoms that do not correlate with imaging findings
In some cases, traditional cervical fusion surgery or another surgical approach may provide better long-term stability or decompression. Careful patient selection remains one of the most important factors in achieving good outcomes.
When Is Surgery Considered?
Most patients should first attempt conservative treatment unless there is severe neurologic compromise. Non-surgical treatment options may include:
- Physical therapy
- Anti-inflammatory medications
- Activity modification
- Epidural steroid injections
- Pain management strategies
Surgery is typically considered when:
- Symptoms persist for weeks or months
- Pain significantly affects daily activities or quality of life
- Progressive weakness develops
- Neurologic deficits worsen
- MRI confirms focal nerve compression
Timing matters. Prolonged nerve compression may reduce the potential for full nerve recovery in some patients.
MRI Findings That Often Support Endoscopic Surgery
Certain imaging findings commonly make cervical endoscopic discectomy a reasonable consideration. These may include:
- Lateral or foraminal disc herniations
- Soft disc protrusions
- Focal nerve root compression
- Limited-level pathology
- Preserved spinal stability
The goal is identifying a specific pain generator that matches the patient’s symptoms and neurologic findings.
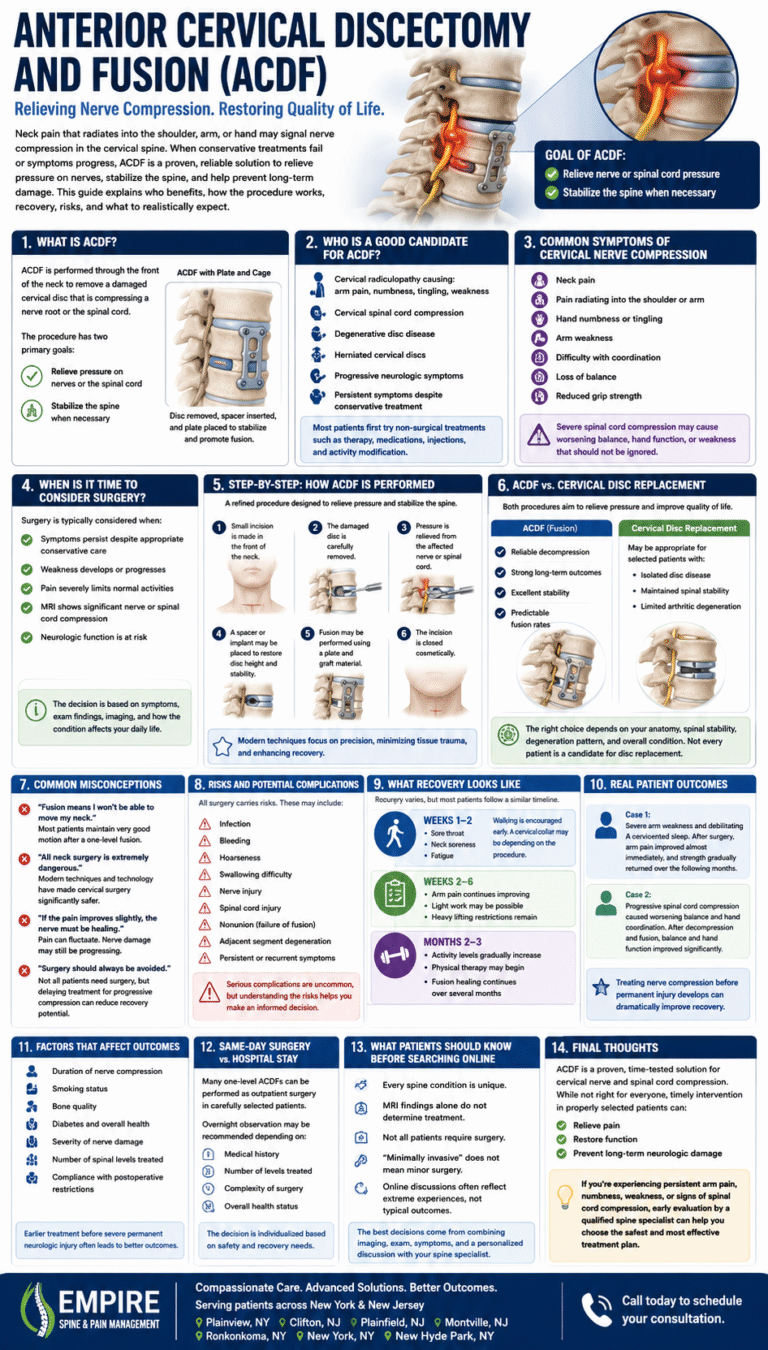
Cervical Endoscopic Discectomy vs Traditional ACDF
Traditional ACDF (anterior cervical discectomy and fusion) remains an excellent and widely performed procedure. However, endoscopic techniques may offer advantages for selected patients. Potential benefits of cervical endoscopic discectomy may include:
- Smaller incision
- Less muscle disruption
- Reduced tissue trauma
- Motion preservation
- Faster recovery
- Less postoperative discomfort
- Earlier return to work and activity
- Reduced need for large implants or hardware in selected cases
Many patients appreciate that minimally invasive surgery focuses on decompressing the affected nerve while preserving surrounding anatomy whenever possible. That said, minimally invasive surgery is not automatically the best option for every patient. The correct procedure depends on the individual anatomy, pathology, and long-term goals.
Common Patient Concerns About Endoscopic Neck Surgery
Many patients are understandably anxious when discussing cervical spine surgery. Common fears include:
- Paralysis or spinal cord injury
- Recurrence of the disc herniation
- Fear of being awake during surgery
- Concerns that minimally invasive surgery is less effective
- Worries about recovery time
Education plays a major role in reducing anxiety. Reviewing imaging together and helping patients understand exactly where the nerve compression is occurring often makes the condition and treatment plan much clearer. A common misconception is that minimally invasive surgery means “smaller” or less complete surgery. In reality, the goal remains the same: achieving effective decompression of the affected nerve while minimizing unnecessary tissue disruption.
What Does Recovery Look Like?
Recovery varies depending on the individual patient, severity of nerve compression, and overall health.
First Few Days
Many patients experience:
- Mild surgical soreness
- Improvement in arm pain relatively quickly
- Early walking and light movement
- Fewer activity restrictions compared to open surgery
First Few Weeks
During the first several weeks:
- Activity gradually increases
- Numbness and weakness may continue improving
- Many patients return to desk work relatively early
- Physical function progressively improves
First Few Months
Nerve healing continues over time. Patients may experience:
- Continued improvement in strength and sensation
- Return to exercise and daily activities
- Ongoing nerve recovery over several months
It is important to understand that nerve healing is often slower than pain relief, especially if nerve compression existed for a prolonged period before surgery.
Risks and Limitations Patients Should Understand
All spine surgery carries risks, including minimally invasive procedures. Potential risks include:
- Infection
- Bleeding
- Nerve injury
- Persistent symptoms
- Recurrent disc herniation
- Incomplete symptom relief
- Need for future surgery
Patients should also understand that the goal is improvement — not perfection. Outcomes depend on many factors, including the duration of nerve compression, overall spinal health, activity level, and individual healing response. Honest discussions about expectations are essential before any surgical decision.
Real Patient Experiences
One patient, a middle-aged professional, developed severe arm pain and weakness from a cervical disc herniation. After conservative treatments including therapy and injections failed, endoscopic decompression was performed. Arm pain improved almost immediately, and strength gradually returned over the following weeks, allowing an earlier-than-expected return to work. Another active patient struggled with debilitating neck and shoulder pain that interfered with sleep and exercise. Following surgery, symptoms improved significantly within days, and the patient resumed light activity within weeks before eventually returning to full activity. While every patient heals differently, these cases highlight the potential benefits of targeted minimally invasive nerve decompression in carefully selected individuals.
Final Thoughts
Cervical endoscopic discectomy represents an important advancement in minimally invasive spine surgery for properly selected patients with cervical nerve compression. For many individuals, the procedure may provide meaningful pain relief, motion preservation, and faster recovery while minimizing disruption to surrounding tissues.
However, successful outcomes depend heavily on accurate diagnosis, careful patient selection, realistic expectations, and choosing the most appropriate treatment approach based on the patient’s unique condition — not simply selecting the newest or least invasive option. ]If persistent neck or arm symptoms are interfering with your quality of life, consulting with an experienced spine specialist can help determine whether cervical endoscopic discectomy or another treatment option may be appropriate for you. Call Empire Spine & Pain Management, we help patients across New York & New Jersey with clinic locations at Plainview, NY • Clifton, NJ • Plainfield, NJ • Montville, NJ • Ronkonkoma, NY • New York, NY • New Hyde Park, NY
Pain treatments are covered by most major medical insurances including Medicare, Workers Comp, No Fault & Others.
Verify your Coverage for FREE
Enter your information below to get started
Your information is encrypted and secure. By submitting this form, you agree to our Communications Terms and Privacy Policy and consent to receive SMS and email communications. You may opt out at any time. We are HIPAA-compliant and value your privacy.

Meet Our Pain Management & Orthopedic Specialists




Dr. Monica Misak
Interventional Pain Specialist

Dr. James Yu, D.O.
Board Certified Anesthesiologist
Board Certified Interventional
Pain Management Physician

Dylan J. O'Rourke
Certified Physician Assistant
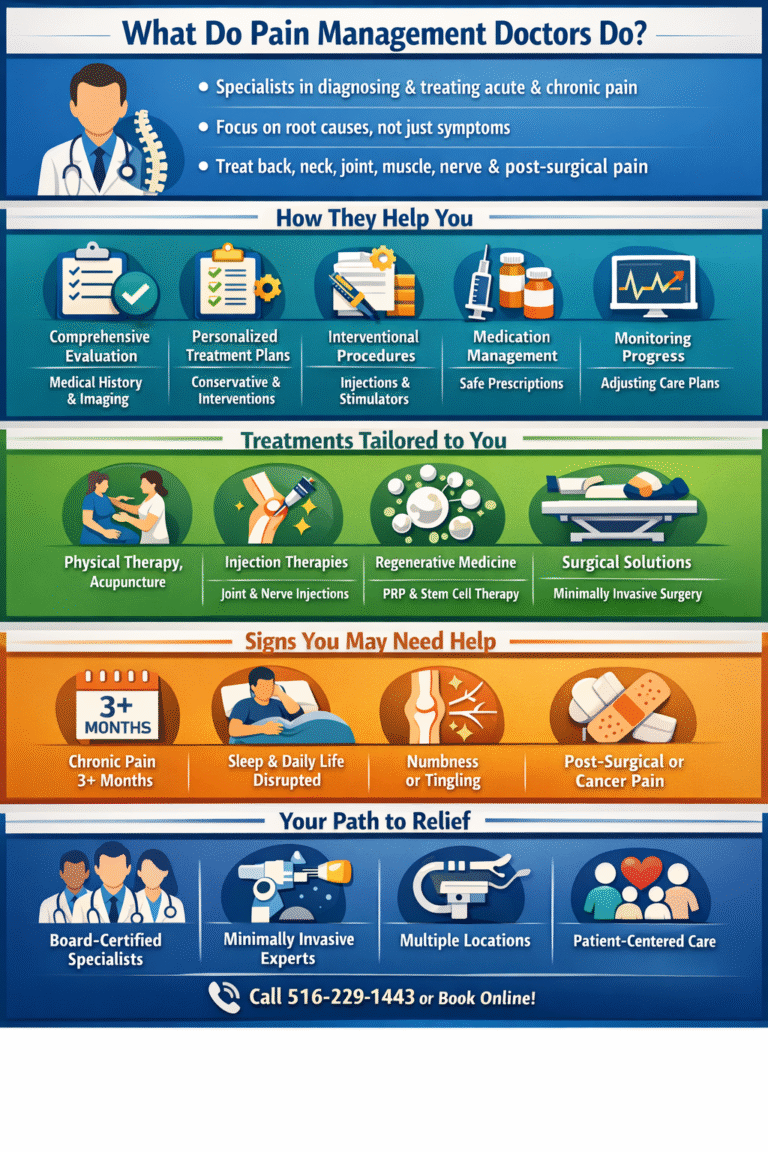
Pain Conditions Affecting Daily Life
Improve your quality of life with our comprehensive approach to pain management
We are dedicated to finding individualized treatment options tailored to fit your needs. Our team is dedicated to helping you lead a productive and active life, free from pain and disruption.
We use an integrative approach to conduct a comprehensive evaluation and assess your condition.
Physical examination and review of your medical history. We assess the cause of your pain, determine its severity and duration, and help you develop an individualized treatment plan.
We provide a range of treatments and procedures to address your chronic pain. These include nerve blocks, injections, physical therapy, implantable therapies and more. We also offer health education to help you better manage your condition.